
California’s Own Evidence Points North
Emundi College of Medicine is being built by people who live in the North State, work in the North State, and know what this region has carried for years. The data matter because they confirm what our communities have long known: the need is greatest here.
When I speak about Emundi College of Medicine, I am not speaking about an abstract idea.
I am speaking about a response that grew out of lived necessity.
Those of us working to create Emundi live here. We work here. Many of us have spent years — in many cases decades — caring for patients in this region, building programs in this region, and watching families do their best in a health care environment that too often asks too much of them.
So when we say the North State needs a long-term solution, we are not guessing. We are describing what this region has lived with for a long time.
The numbers matter because they make that reality visible to others — to policymakers, to philanthropic leaders, and to anyone who wants to understand where the case for investment is strongest.
Across the North State, people know what shortage feels like.
It feels like waiting too long for a primary care appointment. It feels like driving hours for a specialist. It feels like delayed referrals, delayed diagnoses, and the stress of not knowing whether care will be available when you truly need it.
That is one of the reasons Emundi exists.

“The data matter because they confirm what our communities have long known: the need is greatest here.”
What the data confirms
And when you look at the data, the picture becomes unmistakable.
The California Health Care Foundation’s 2026 report on the primary care workforce notes that more than 11.4 million Californians — more than one-quarter of the state’s population — live in federally designated primary care shortage areas. It also finds that if we tried to meet all recommended care using a physician-only model, it would require 26.7 hours of work per day from a single primary care doctor. In other words, the shortage is real, and the old model is not enough.
But the most important point for our purpose is this: the shortage is not evenly distributed across California.
“The shortage is not evenly distributed across California.”
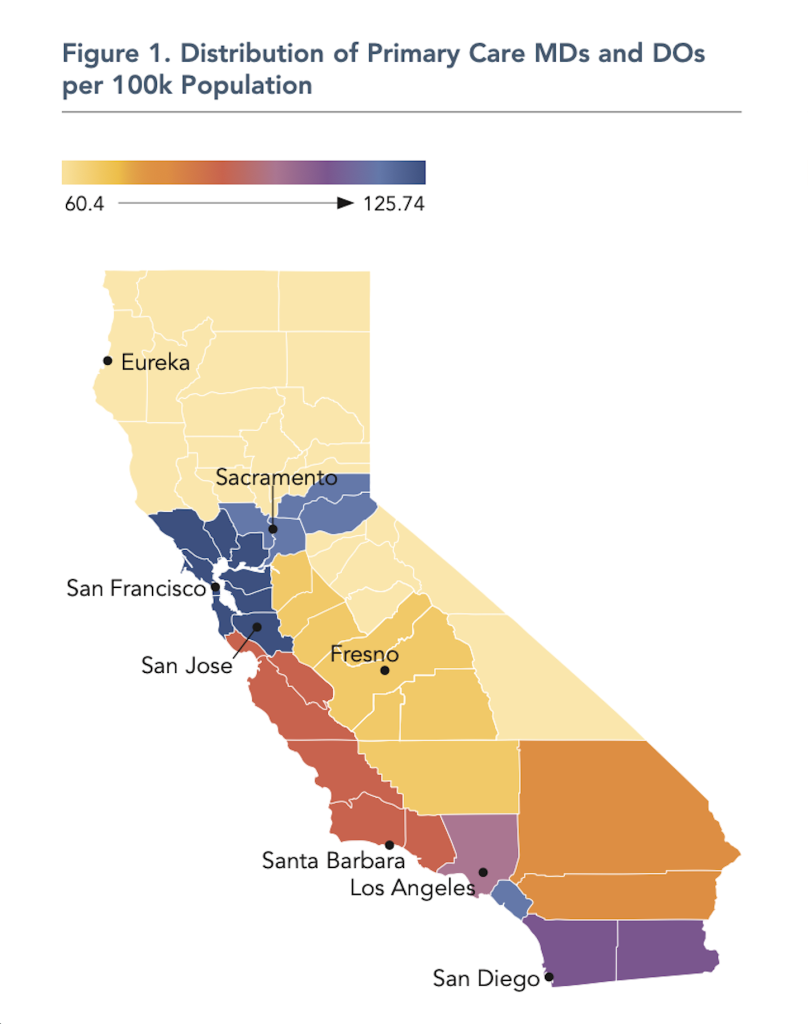
That is why Figure 1 in the CHCF report makes the picture plain. It does not create the case for the North State. It confirms it. The map shows that the Northern/Sierra region has the lowest concentration of primary care MDs and DOs in the state. It also shows that this region has the oldest primary care physician workforce, along with relatively low supplies of nurses, pharmacists, and behavioral health professionals.
That is not a minor regional variation.
That is a warning.
And it helps explain why the North State experiences this challenge not as an inconvenience, but as a strain on the whole system: hours of travel for care, months on waiting lists, and workforce shortages that quickly become access problems for entire communities.
Behavioral health adds another layer of urgency.
HCAI projects that all 58 California counties face psychiatrist shortages, with some of the most severe shortages concentrated in the Northern & Sierra region. Statewide, the projected need is 3,782 additional psychiatrists in 2025, rising to more than 6,200 by 2033.
And there is another problem unfolding inside the shortage: replacement.
The CHCF workforce report notes that only about two-thirds of physicians, physician assistants, and nurse practitioners in primary care specialties are actually providing outpatient patient care 20 or more hours per week. It also notes that 15% of primary care physicians doing that level of care are already age 65 or older, and it projects a statewide shortage of 7,229 primary care physicians by 2035.
So this is not simply a matter of being short today.
It is also a matter of whether regions like ours will have enough physicians tomorrow.
CHCF’s March 2026 note on California’s Rural North puts the broader regional picture in equally clear terms. It describes a region spanning about 39,000 square miles and home to 1.1 million residents. It finds the Rural North has some of the steepest health care challenges in California, with 69% of residents saying health care costs are rising faster than income, more than 70% saying they have skipped doctor visits because of cost, more than half carrying medical debt, and the region having only about two-thirds as many physicians per 100,000 people as the state overall.
Why recruitment alone is not enough
That is why this conversation has to be larger than recruitment alone.
Recruitment matters. Loan repayment matters. Telehealth matters. Residency growth matters. But a region that relies only on importing physicians from somewhere else will remain vulnerable if it does not also build a stronger way to grow and keep more of its own workforce.
That is the deeper rationale for Emundi College of Medicine.
Emundi is being developed because the people closest to this problem have lived with it, worked inside it, and come together around the need for a long-term answer.
And what is striking is that CHCF’s recommendations point in exactly that direction. The report calls for expanding pipeline and apprenticeship programs for rural and underserved regions, supporting programs that help students complete training more quickly, providing scholarships and loan repayment for primary care service in shortage areas — especially rural areas — and giving greater weight to rurality in workforce development decisions.
That is also why Emundi is thinking beyond the traditional starting point of medical school alone. We intend to create a stronger and more efficient path into medicine, including a bachelor’s-to-MD track, so that qualified students can move earlier and more intentionally toward becoming physicians while staying connected to the communities that need them most. In a region like ours, the path into medicine cannot begin only at the doors of a medical school. It has to begin earlier.

“In a region like ours, the path into medicine cannot begin only at the doors of a medical school. It has to begin earlier.”
In other words, the answer is not only more funding somewhere.
It is purposeful infrastructure built where the need is greatest.
What Emundi is being built to do
That is how we think about Emundi.
A medical school should not be understood only as a place where students sit in classrooms and earn degrees. At its best, it becomes part of a regional ecosystem. It creates pathways for local students. It strengthens teaching relationships with hospitals and clinics. It supports residency growth. It brings academic seriousness to regional health care questions. And over time, it helps shape a workforce more likely to understand the communities it serves because it trained among them.
That is especially important in the North State.
This region is not one city. It is a geography of regional referral centers, rural hospitals, agricultural communities, mountain counties, coastal communities, community clinics, and towns that are often asked to do too much with too little. A medical school for this region has to be built with those realities in mind. It has to be community-rooted, regionally accountable, and designed for the practical conditions of rural and regional medicine.
That is the vision behind Emundi.
No one institution will solve every problem by itself.
But a serious, community-rooted medical school can help anchor a larger solution — one that includes physician education, clinical partnership, rural training, residency development, and a stronger long-term workforce strategy for Northern California.
Why this matters now
That is why this project exists.
The North State does not need to be reminded that it is resilient. It already is.
What it needs is sustained investment in its future.
And one of the clearest ways to make that investment is to help build a medical school with the region, for the region, and accountable to the communities it is meant to serve.
If donors and policymakers want to invest where the case is strongest, they do not have to guess.
“California’s own evidence points north.”
Subscribe to Emundi Insights
Receive future essays, updates, and report releases from the Emundi Foundation.



